Technology is changing every aspect of clinical trials and although change is happening slower than many want, 2020 is still likely to see huge development and innovation.
In April 2019, we surveyed clinical trials professionals around the world on how they saw the current state of the industry and where they thought it was going in the next few years. Based on 214 responses, the final report was introduced byCiteline, picking out some of the key trends:
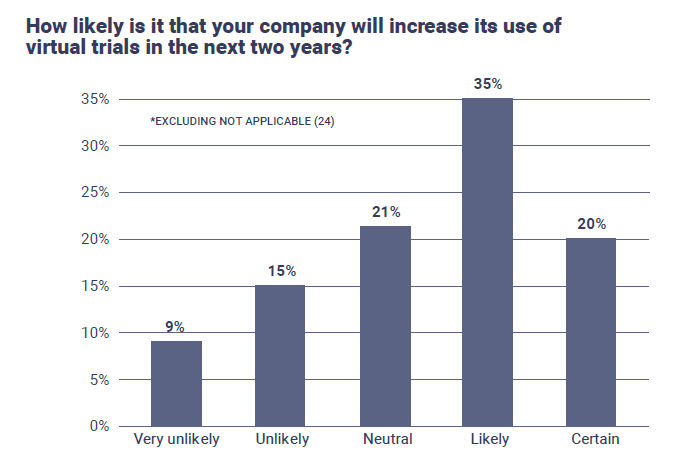
“Patient centric approaches are expected to reap many benefits and technologies are key to realizing these benefits. Virtual trials could increase patient participation and provide enhanced efficiencies in data monitoring/analysis. Asia and N. America are ahead of Europe in employing this approach, but virtual trials are expected to increase in the next two years across all regions. Wearables and sensors improve real-time data acquisition and, for some respondents, data quality. However, data quality remains a concern for some, which is second only to data privacy/security concerns.
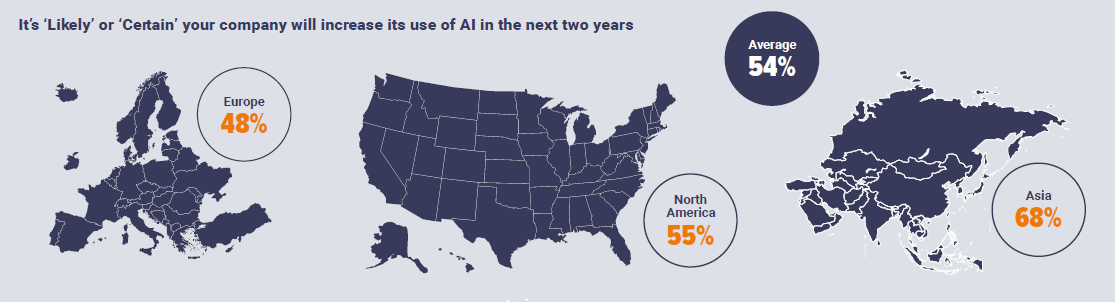
Currently, AI is seldom used in trials, but increase usage is anticipated during the next two years. Robotic Process Automation (RPA), Natural Language Processing (NLP) and eHealth records offer the largest benefits, presumably for data management. For early phase studies, AI utilization may serve a more analytical role for patient identification/stratification and predictive purposes.
Study design improvements for early phase protocols aim to achieve meaningful outcomes in a shorter time. Innovative designs most commonly utilize adaptive designs, while umbrella, basket and platform designs often are employed and protocol changes for QT safety studies already are used in ~25% in early phase studies. Use of ‘real world’ evidence is increasingly important as industry addresses regulatory agencies’ post-marketing requirements and provides support for new drug applications. Cost and time savings should be realized by utilizing ‘real world’ evidence. Currently, N. America and Asia utilize this data more fully than does Europe.”
Download the full Clinical Trials State of the Industry Report here.
Alongside the report, we asked 10 clinical trials professionals from pharma, technology providers, patient groups and biotech for their one prediction for how clinical trials will most change in 2020:
“Sourcing/outsourcing will be supported by more automated systems by 2020 and sponsors will mainly do oversight and less micro-management since both CROs and Sponsors will join the same most common technology. This will allow sponsors to be more efficient in resourcing internally and avoid duplication of task by both CRO and sponsor. Non-core activities will be delegated to CROs who are becoming the experts, whilst science will stay core at the sponsor. Probably support from ad hoc consultancy will be part of the main business and become more efficient and cost effective including in science support.”
“I don’t expect revolutionary changes. The trend towards more data-driven decisions regarding inclusion/exclusion criteria, country and in particular site selections will continue, reducing the dependence on know-how and experience of individuals. I hope we get a better understanding of the impact of trial complexity, in particular protocol complexity, on our ability to execute our clinical trials according to plan. We will see more efforts towards virtual/digital trials, but this will be a slow shift.”
“The change I want to see is the industry focusing on relieving the burden on patients. The good news is technology need no longer be a barrier. The next step is to better design studies around patients, rather than looking for mythical patients that fit a particular protocol.”
“Trials ongoing in 2020 need to be developed now, and as such I think two of the largest changes are likely to relate to. Firstly, computer-enhanced patient identification. And secondly, an increase in the number of trials exploring drugs that also incorporate devices to optimise patient behaviour with those medications. These have potential to increase benefits of treatment, as well as monitor or mitigate some of the adverse effects, thereby rapidly improving potential patient benefit with technologies already available.”
“I'm not sure, given we're already nearing the end of 2019, that we'll see a huge shift in the next 15 months. However, it's increasingly hard to ignore the transfer of wearables from the world of consumer health (where they carry disclaimers about not being medical devices) into clinical research. The recent Apple announcement of three observational trials with major US health providers, organised around its watch and Research app, attracted a lot of attention, and it seems a welcome inevitability that trial protocols will increasingly look to wearables (and other solutions) for opportunities to minimise in-person site visits.
Certainly, talk about virtual and hybrid trials is everywhere. Exactly how far that trend moves from press release to regular reality by the end of next year remains to be seen, but it's certainly happening.”
“I think we will see an increase in utilisation of wearables to supplement data that is captured formally by the physician.”
“We have seen the adoption of digital inhalers in clinical trials. Today’s connected device for injectables is not that user friendly, but I do see a few that are integrated, low cost and easily applied to both trials and commercial. They can help clinical trials become more robust, ensuring adherence and compliance to the treatment regimen. Key to those systems is that they are integrated and capture just the essential information. They have the capability to provide a seamless user experience and benefit all the stakeholders (patients, pharma, health insurance / payers, HCP).”
“In the oncology area, new treatments are getting more and more personalized. This indicates that we need to collect and analyze various biomarkers without solid evidence that each specific biomarker is of interest for the specific indication tested. I see that more tissue samples are being taken to possibly gain knowledge of how to provide tailor made therapies, even in phase III pivotal trials. This causes increased workload for sites and study teams that needs be accounted for.”
“More devices being added to clinical trials, some of which will be useful and work and some that won’t – not necessarily because they don’t work but because patients won’t use them. The critical success factor will be patient acceptability. If the device means that they need to do more (eg taking their own samples, wearing a device) then there has to be something in it for them and for the clinical team at the sites.”